April 28,2021
Short case - GENERAL MEDICINE
45 year old male, resident of ramanapet, farmer by occupation, came to the Opd, with chief complaints of
shortness of breath since one year.
Bilateral pedal edema since three months.
HISTORY OF PRESENT ILLNESS:
The patient also complains of pedal edema since 3 months, insidious in onset, gradually progressive from involving the ankle to involving the whole limbs, pitting type, aggravated by walking , slight in the morning and more by the end of the day which relieved on elevating the legs.
Patient also gives a history of decreased urine output since 1 month, insidious onset, gradually progressive.
There's history of weight loss.
No h/o paroxysomal nocturnal dyspnea.
No history of cough and expectoration, chest pain, no history of palpitations and syncope .No history of fever, sore throat, joint pains. No hemoptysis, hematemesis, no history of Jaundice, no history of burning micturition.
PAST HISTORY:
He had a road traffic accident 3 years back, had a surgery on right leg and was on medications for one year (analgesics).
He is a known case of hypertension since 2 years, diagnosed when he went to a camp- was using nicardia 20 MG thrice daily and stop taking tablets since one year.
The patient is on dialysis since 10 months.
He is not a known case of diabetes, TB asthma, epilepsy.
PERSONAL HISTORY:
He has a mixed diet.
Appetite- normal
Sleep- disturbed
Bladder- irregular
Bowel movements- regular
Addictions- chronic alcoholic for 20 years stopped drinking since last three years.
FAMILY HISTORY:
There is no significant family history.
DRUG HISTORY:
The patient used analgesics for a year.
Used nicardia 20 MG for Hypertension.
GENERAL EXAMINATION:
The patient is conscious, coherent, Cooperative, moderately built and nourished.
Pallor - present
There are no signs of icterus, cyanosis, koilonychia, clubbing and lymph adenopathy.
Edema- present.
JVP- raised.



VITALS:


Palpation
no local rise in temperature
no tenderness
no guarding and rigidity
no palpable masses.
Percussion:
shifting dullness- present
liver span-normal
Auscultation:
bowel sounds are heard.
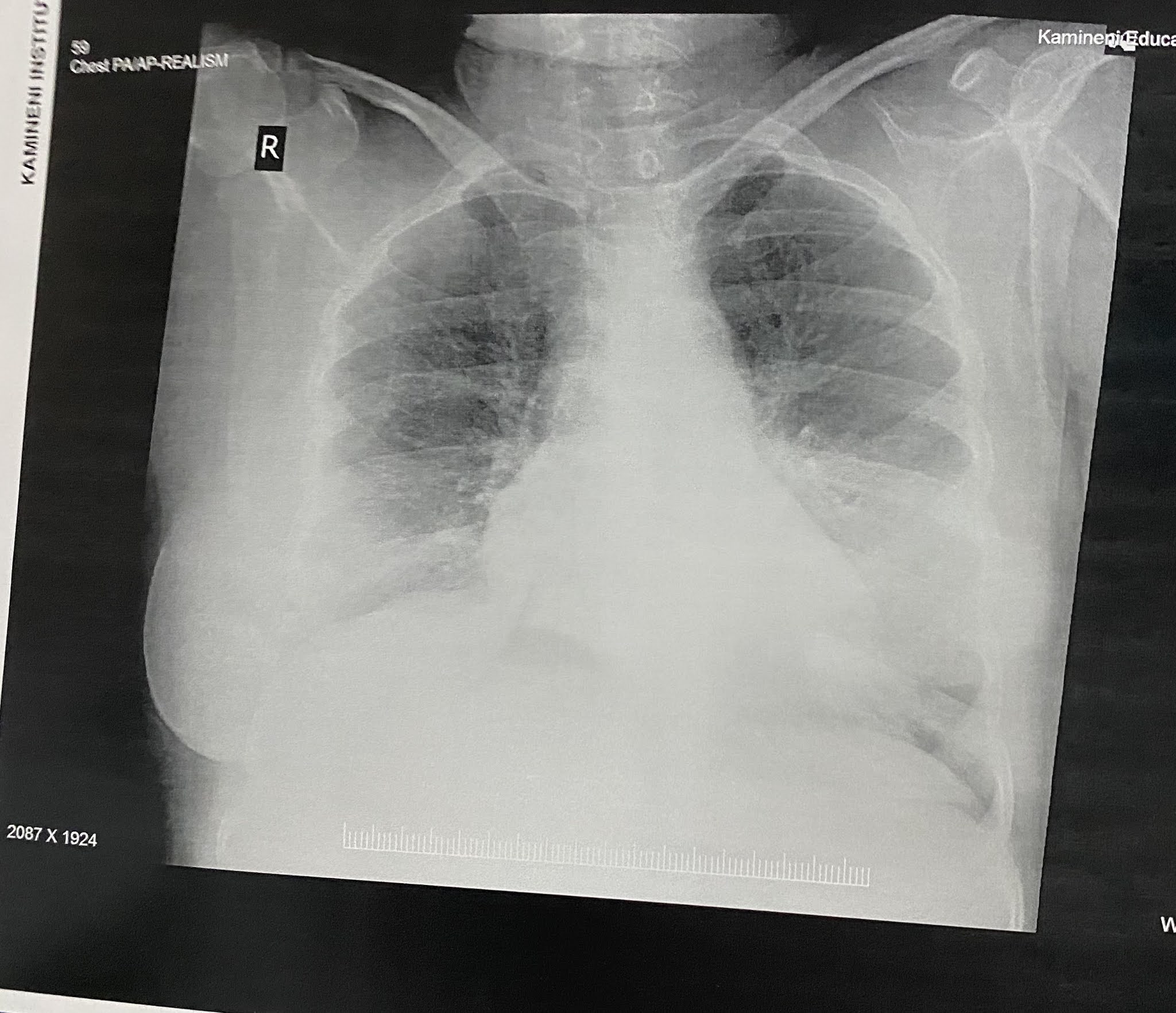
Respiratory system :
bilateral air entry- present
normal vesicular breath sounds heard
basal crepitations present in both the lung fields.
Central nervous system- normal.
INVESTIGATIONS:
CBP-
Hemoglobin- reduced
PCV- reduced
RBC count -reduced

CUE-
Albumin in urine




RFT:
Serum urea and creatinine- raised.

LFT:

SERUM IRON:

Grade-II renal parenchymal disease

PROVISIONAL DIAGNOSIS:
CHRONIC KIDNEY DISEASE WITH HEART FAILURE.
TREATMENT:
Salt and fluid restriction
Tab. Nicardia 10mg T.I.D
Tab. Lasix 40mg B.D
Tab. Arkamin 100mg
Tab. Unifer
Capsule. Gel cal D3








{kind=link}